Dr Boullosa’s forgotten pieces don’t fit the puzzle
Martin Buchheit and Paul B. Laursen
(to be published soon in Sports Med in response to Dr Boullosa’s letter)
We appreciate the opportunity to respond to Dr Boullosa’s letter of concern [1] on issues brought forth in our 2-part review on high-intensity interval training (HIT) [2, 3]. However, we were surprised to read the letter’s content, feeling generally that most comments were off-topic, and accordingly offering little to assist the practitioner. Nevertheless, we will use this opportunity to elaborate on certain principles and in doing so outline why his so-called ‘forgotten pieces’ do not fit the training program puzzle.
His first critique of our review [2] was that there was no comment as to how progressive exercise test protocol design influences the relationship between the velocity/power at maximal oxygen uptake (v/pO2max) and performance. This is simply incorrect. Section 2.5 of our review extends to more than a full page of printed text describing in detail the history, theory, as well as measurement techniques practitioners can perform in both the laboratory and the field to determine appropriate values, as well as their limitations. We state clearly how “vO2max [determination] is method-[4] and protocol-dependent [5]”. It would therefore be implied that the magnitude of the relationship between vO2max and performance would comparatively be affected. We did not elaborate further on this point, as such discourse would be superfluous within the context of the review, which focused on HIT prescription, and not performance prediction. For these reasons, Dr Boullosa’s first piece doesn’t fit.
His second critique was that “there was no reference […] to how [anaerobic speed reserve] ASR could be influenced by the method [used] for [maximal sprinting speed] MSS determination”. While the point is valid, there are a limited number of known methods for determining MSS, and these unlikely produce differences in MSS as great as those seen with vO2max or the final speed reached during incremental test (VIncTest) [2]. In practice, the use of a flying 10- [6] or 20-m [7, 8] time is probably the most common method of determination, although peak instantaneous speed can also be measured now with radar gun technology [9]. The difference between these methods is generally less than ~2% (personal observations), which is substantially lower than the possible ~20% difference that can be observed for vO2max/VIncTest determination [2]. Moreover, the typical error of measurement for MSS (1%) is also clearly lower than that of VIncTest (3.5%) [10]. Taken together, these data show that the determination of ASR is less likely to be affected by variations in MSS compared with vO2max/VIncTest estimation, and explain why we chose against elaborating further on this point in our review [2].
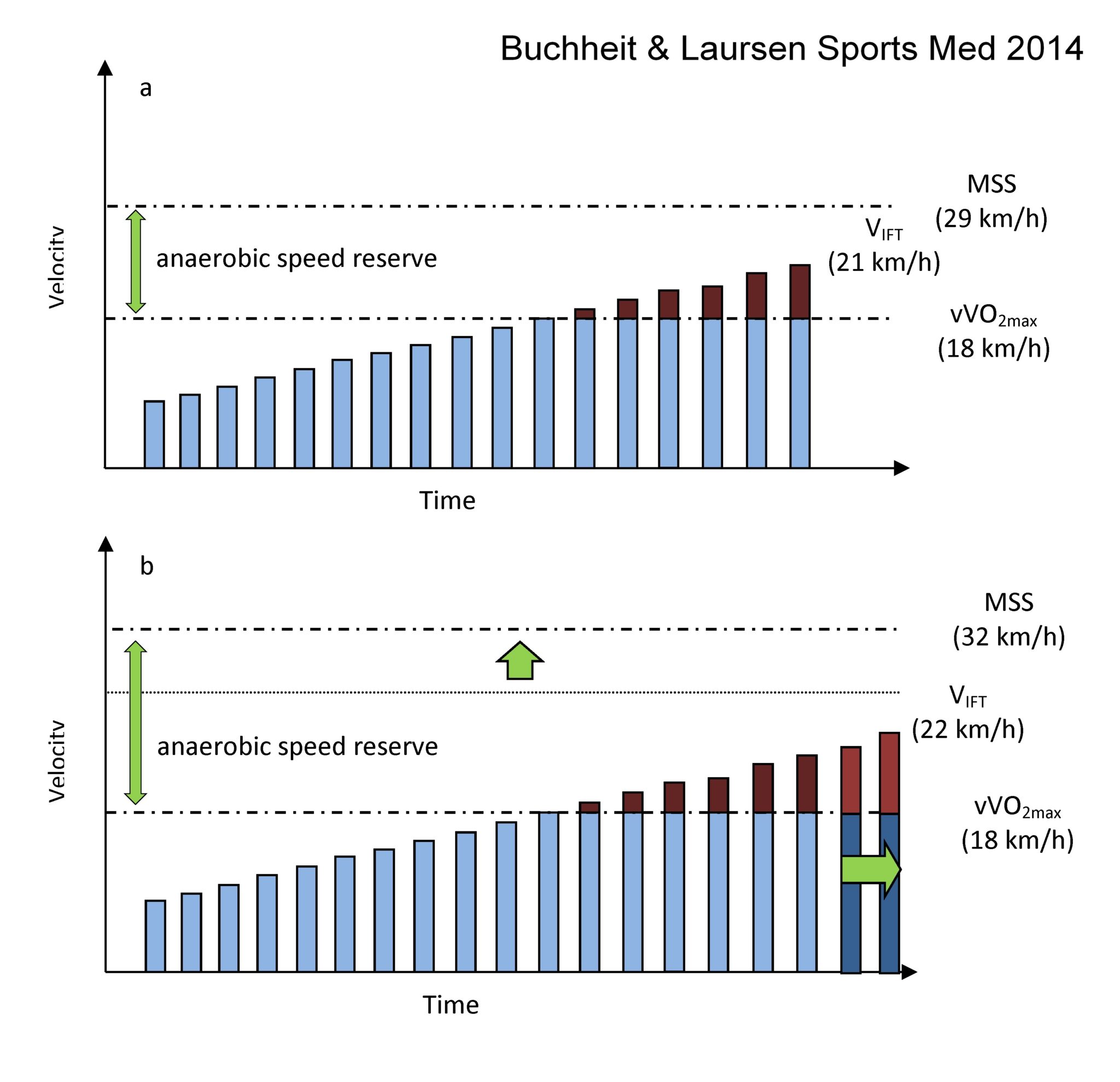
Dr Boullosa goes on to claim that “the practicality of the 30-15 Intermittent Fitness Test (30-15IFT) for evaluating simultaneously different locomotor abilities and ASR is contradictory stricto sensu with the previous definition of ASR”, and offers instead “a potentially simple and time-saving alternative evaluation of ASR with the recording of a maximum sprint test performed 3-5 min after an incremental test for vO2max determination [7].” The first part of the comment is unclear to us, since it is now known that VIFT is sensitive to both vO2max/VIncTest and MSS [11]. The ‘dual sensitivity’ of the 30-15IFT motivated our comments around the ‘simultaneous’ evaluation of different locomotor abilities. We showed that while the first determinant of VIFT is vO2max/VIncTest, MSS is likely to be the secondary influencing variable [11]. If we take, for example, two young football players presenting with similar v O2max/VIncTest scores, the athlete with the faster MSS also has the faster VIFT (Figure 1, personal data). The other part of Dr Boullosa’s comment suggesting assessment of MSS following the incremental test is also at odds with the current practices that we are personally aware of, both for team sports and distance running. While standing [12] and flying [7, 8] 20-m sprint tests have been used in the literature with endurance athletes after exhaustive exercise, such procedures are problematic for assessing MSS (i.e., 10-m splits likely allow a better assessment compared with 20-m ones, and the fastest split is not necessarily derived from the last one [6]). Since athletes must sprint maximally over at least 40-to-50m to ensure their MSS is captured, coaches (irrespective of the sport) tend to be (in our experience) reluctant to assess MSS post-incremental test, mainly due to the increased hamstring and adductor injury risk [13]. The assessment of MSS following an incremental test is also questionable from a performance standpoint, since MSS could potentially be impaired, especially in team-sport athletes. While some endurance athletes might maintain sprinting speed [14], the magnitude of the performance decrement post-exhaustive effort is largely and inversely correlated with initial sprinting speed [8]; faster team sport players therefore would likely incur a large impairment to MSS using such an approach. Since this potentially serious effect is athlete-background and locomotor profile-dependent, it makes more sense practically to assess MSS on a separate occasion, when all athletes have recovered from the vO2max/VIncTest [11, 15]. In light of these arguments, we believe Dr Boullosa’s second piece does not fit the puzzle.
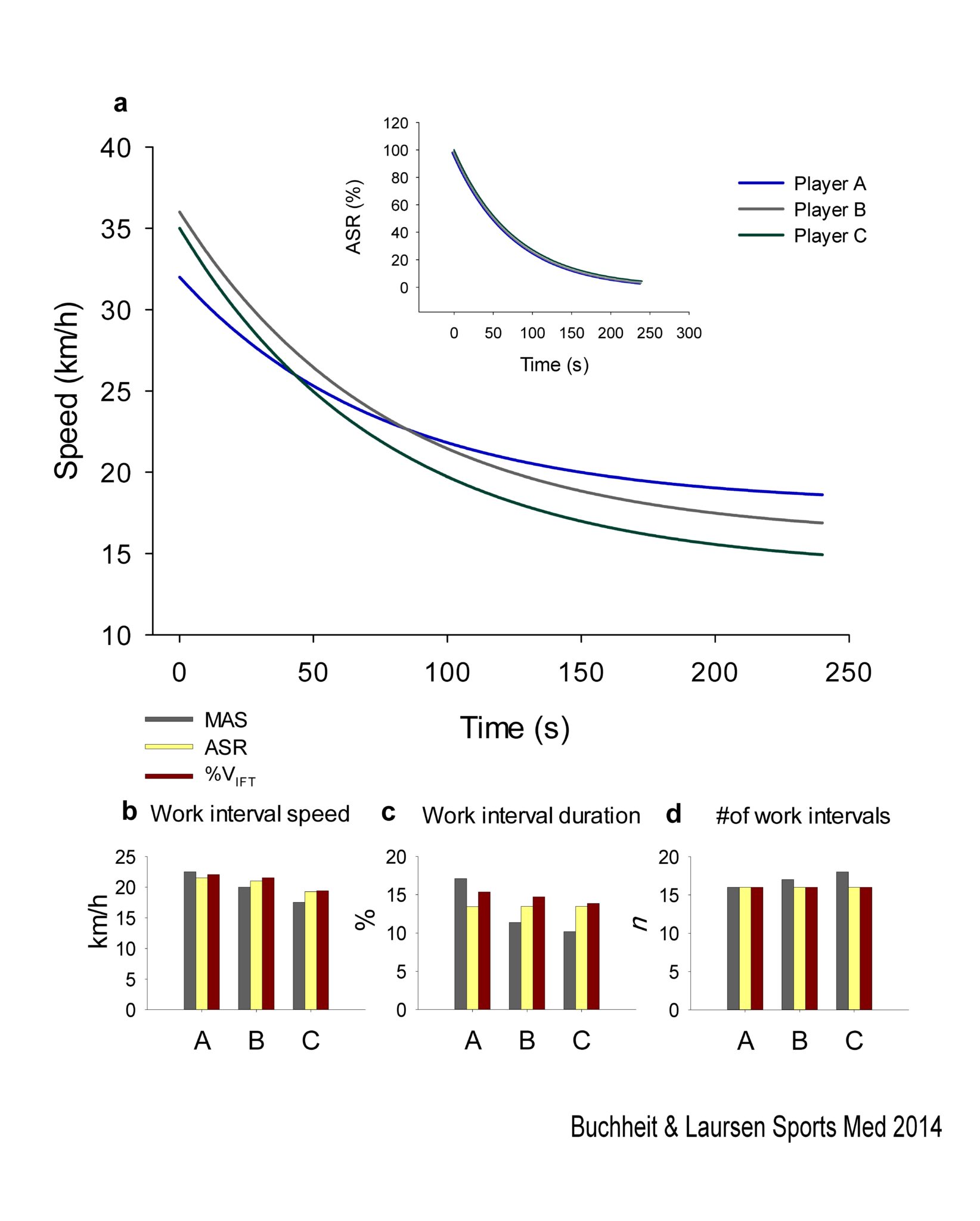
In Dr Boullosa’s third critique, he states that “there is no actual evidence supporting the usefulness of ASR for individualizing training intensity prescription.” While we agree that a comprehensive study comparing the acute and long-term physiological and performance responses of HIT sessions based on vO2max/VIncTest vs. %ASR has yet to be published, we can provide evidence to support the use of this method to individualize HIT (Figure 2). First, the approach is used across a considerable number of (team) sports worldwide, and has been now for more than 10 years, which is proof of its practicality, interest and usefulness (i.e., ‘best practice’ theory). Second, the ASR approach is taught in well-established and respected strength and conditioning courses throughout the world (e.g., France, Spain, Italy, Germany, Switzerland, USA, Australia, New Zealand), and has been the subject matter of publications by other groups (e.g., [16]). Last, as with the smaller between-athlete variations in acute cardiac responses to VIFT vs. vO2max/VIncTest -based HIT sessions [17], we have observed a smaller between-athlete variation in time-to-exhaustion using % of ASR compared to % of v O2max/VIncTest (31 vs. 55% during a 15s @ 95% VIFT / 15s passive HIT, unpublished data). This clearly shows that using the entire locomotor profile (or at least VIFT) to prescribe running-based HIT with short intervals, rather than only vO2max, allows the standardisation of relative exercise intensity at the individual level. The direct consequence of this intensity standardisation is that the work interval duration represents a constant fraction of the predicted time to exhaustion at this relative intensity for all athletes. Along these lines, the number of work intervals required to match the predicted supramaximal distance capacity remains also constant for all athletes (Figure 2).
Dr Boullosa goes on to emphasize that “the improvement of both MSS and vO2max are independent objectives that depend on the requirements of a specific sport”. We of course concur, as we highlighted in Figure 1 from the first part of our review [2], where we outline how training objectives should relate to the athlete’s profile, sport and training cycle. But we did not suggest that variation in HIT formats can be used specifically to improve either MSS or vO2max in isolation. It is clear that if the training objective is to improve MSS, isolated speed/strength sessions would be recommended, and not HIT sessions [18, 19], as shown also in Figure 1 of the first part of the review [2]. In addition, the remaining part of Dr Boullosa’s comment, where reference is made to acceleration capacity in team sports, shows that he fails to consider separately the physiological and neuromuscular requirements of 1) a given training session aimed at improving an athlete’s physiology and 2) competitive situations. While the principle of training specificity should not be forgotten, excessive reliance on competition-like training content (e.g., match replication) has its limitations [20, 21]. The main interest in determining ASR is to account for the athletes’ entire locomotor profile when performing a run-based HIT session at high but not maximal speed, which has implications for acute physiological and performance responses during the session (see previous point), irrespective of the sport demands. Similarly, the value of maximal acceleration capacity, although unlikely to be reached during HIT, may eventually be considered with respect to the frequent start-and-stop requirements of HIT with short intervals [22], but again, without direct link to the actual sport demands. Finally, while MSS is not often reached during matches [23], a faster MSS likely reduces relative neuromuscular load [15, 24], which may improve exercise tolerance and lower injury risk. Along these lines, although outside the scope of our review, the development of MSS as a training focus for team sport athletes makes logical sense, and is probably as important as acceleration capacity. Regardless, we again have an odd-shaped puzzle piece offering from Dr Boullosa’s that we can’t make fit.
He further states that we have a “misunderstanding [of] post-activation potentiation (PAP) after different HIT modalities”, where we suggest that “around vO2max intensities PAP would be maximized, thus favoring a positive neuromuscular loading”. Dr Boullosa might have himself misunderstood our conclusions, since we were not implying a causal link between the potential PAP effect and positive neuromuscular loading. We in fact refer to “long-term structural adaptations that allow fatigue-resistance to high-speed running [25]” as a separate mechanism (section 2.2.6). Indeed, the 80% of vO2max threshold he refers to for maximising PAP actually falls within the blue zone of our Figure 5 in the second part of the review (~80-85% v O2max, see text in the 2.2.6 section [3]). While his suggestion of a likely beneficial effect of recovery intervals for neuromuscular fatigue development during HIT may be true when comparing continuous versus intermittent incremental tests, the results we show in Figure 2 (b panel) from the 2nd part of our review suggest otherwise [3]. For instance, the repeated-sprint exercise (5s/25s) associated with the greater CMJ performance impairment, included a longer relief interval than the HIT with short interval session (10s/20s), where an increase, and not a decrease in CMJ performance was observed. This suggests that the neuromuscular responses to high-intensity exercise may reflect the combined influence of both work and relief interval characteristics, with work interval intensity the likely major contributor. Indeed, it is well established that it is the intensity and duration of the work interval, and not the average HIT intensity, that determines the largest portion of the physiological, perceptual and performance responses to a given HIT session [26-29]. Following these lines, the mention by Dr Boullosa of the so-called ‘new’ equation proposed by Tschakert and Hofmann (already proposed by Billat nearly 15 years ago [30]) aimed at equating HIT sessions based on external workload, also becomes a puzzle piece that will not interlock.
Dr Boullosa ends his letter stating how “the practicality of the [HIT] programming examples provided in [our] review [are] limited without knowing the outcomes of different physical capacities” and that “it is necessary to study […] the whole training workload [and] consider the […] other training exercises, including any form of physical activity as recently suggested [31].” His first comment is perplexing to us, since the four HIT programming examples we provided from different elite sport athlete programs (Tables 4 to 7 of the second part of the review [3]) were shown over different training cycles, so as to illustrate how HIT manipulation can be related to different physiological (e.g., VO2 development) and performance phases. Providing more detailed recommendations would, of course, be hazardous, and, in fact, impossible, since there would be as many options for training program content as there are athletes in the world (Figure 1 of the first part of the review [2]). The idea of considering the “whole training workload” is reflected throughout our review, where we consistently emphasize how HIT programming needs to be considered within the context of all training content, from skill and speed/strength sessions, to low intensity continuous work, to threshold sessions, to O2 work, to supramaximal training, to individual athlete characteristics, to recovery, etc. – this, of course, is the complex and dynamic “Puzzle” we continually strive to solve! Reference made by Dr Boullosa to the single study of Faude et al. [32], suggesting a greater benefit of high volume training compared with HIT, is at odds with his aforementioned comment on the presumed importance of equated external workload amongst training sessions, as training load was in fact more than 70% greater in the high volume training compared with the HIT group. As cited by Dr Boullosa himself in one of his own publications [33], there are dozens of other studies showing the more favourable responses with HIT. If we were to reference a single study of best practice today, we would quote that of Stoggl and Sperlich, who concluded that a mixture of all types of training may be the most efficient approach [34]. Finally, the last sentence of Dr Boullosa’s letter, referring again to his work [31] brings up our last point, whereby throughout his letter there appears to be an undue emphasis on his own work (40% of cited papers in his letter [1]), since the importance of actual physical activity as an interference mechanism with respect to longitudinal adaptations was suggested more than 10 years ago in adults [35] and children [36] subjected to a training intervention.
While we appreciate the opportunity that Dr Boullosa’s letter has provided to us to explain further some of the concepts within our 2-part review, we hope we have made clear how his so-called forgotten pieces do not fit within a practitioner’s training program puzzle.
References
- Boullosa DA. The forgotten pieces of the high intensity interval training
Puzzle. Sports Med. 2014: In press.
- Buchheit M and Laursen PB. High-intensity interval training, solutions to the programming puzzle: Part I: cardiopulmonary emphasis. Sports Med. 2013;(43):313-338.
- Buchheit M and Laursen PB. High-intensity interval training, solutions to the programming puzzle. Part II: anaerobic energy, neuromuscular load and practical applications. Sports Med. 2013: In press.
- Hill DW and Rowell AL. Running velocity at VO2max. Med Sci Sports Exerc. 1996;(28):114-119.
- Midgley AW, McNaughton LR, and Carroll S. Time at VO2max during intermittent treadmill running: test protocol dependent or methodological artefact? Int J Sports Med. 2007;(28):934-939.
- Buchheit M, Simpson BM, Peltola E, et al. Assessing maximal sprinting speed in highly-trained young soccer players. Int J Sports Physiol Perform. 2012;(7):76-78.
- Boullosa DA, Tuimil JL, Alegre LM, et al. Concurrent fatigue and potentiation in endurance athletes. Int J Sports Physiol Perform. 2011;(6):82-93.
- Nummela AT, Heath KA, Paavolainen LM, et al. Fatigue during a 5-km running time trial. Int J Sports Med. 2008;(29):738-745.
- Impellizzeri FM, Marcora SM, Castagna C, et al. Physiological and performance effects of generic versus specific aerobic training in soccer players. Int J Sports Med. 2006;(27):483-492.
- Buchheit M and Mendez-Villanueva A. Reliability and stability of anthropometric and performance measures in highly-trained young soccer players: effect of age and maturation. J Sports Sci. 2013;(31):1332-1343.
- Buchheit M and Mendez-Villaneuva A. Supramaximal intermittent running performance in relation to age and locomotor profile in highly-trained young soccer players. J Sports Sci. 2013;(31):1402-1411.
- Buchheit M, Kuitunen S, Voss SC, et al. Physiological strain associated with high-intensity hypoxic intervals in highly trained young runners. J Strength Cond Res. 2012;(26):94-105.
- Small K, McNaughton LR, Greig M, et al. Soccer fatigue, sprinting and hamstring injury risk. Int J Sports Med. 2009;(30):573-578.
- Boullosa DA and Tuimil JL. Postactivation potentiation in distance runners after two different field running protocols. J Strength Cond Res. 2009;(23):1560-1565.
- Mendez-Villanueva A, Buchheit M, Simpson BM, et al. Match play intensity distribution in youth soccer. Int J Sport Med. 2013;(34):101-110.
- Heaney N and Willey B. The efficacy of utilising the anaerobic speed reserve to prescribe supramaximal high intensity interval training with elite female hockey players. In Australian Strength & Conditioning Association Conference. Melbourne, 2013.
- Buchheit M. The 30-15 Intermittent Fitness Test: accuracy for individualizing interval training of young intermittent sport players. J Strength Cond Res. 2008;(22):365-374.
- Buchheit M. Should we be recommending repeated sprints to improve repeated-sprint performance? Sports Med. 2012;(42):169-172.
- Haugen T, Tonnessen E, Hisdal J, et al. The role and development of sprinting speed in soccer. Int J Sports Physiol Perform. 2013: Aug 27. [Epub ahead of print].
- Mendez-Villanueva A and Buchheit M. Football-specific fitness testing: adding value or confirming the evidence? J Sports Sci. 2013;(31):1503-1508.
- Hervert SR, Sinclair K, and Deakin GB. Does skill only conditioning help improve physiological and functional fitness in amateur soccer players? J Aust Strength Cond. 2013;(21):34-36.
- Dupont G, Blondel N, and Berthoin S. Performance for short intermittent runs: active recovery vs. passive recovery. Eur J Appl Physiol. 2003;(89):548-554.
- Mendez-Villanueva A, Buchheit M, Simpson B, et al. Does on-field sprinting performance in young soccer players depend on how fast they can run or how fast they do run? J Strength Cond Res. 2011;(25):2634-2638.
- Buchheit M, Simpson BM, and Mendez-Villaneuva A. Repeated high-speed activities during youth soccer games in relation to changes in maximal sprinting and aerobic speeds. Int J sport Med. 2012;(34):40-48.
- Rusko HK, Tikkanen HO, and Peltonen JE. Altitude and endurance training. J Sports Sci. 2004;(22):928-944; discussion 945.
- Billat LV, Slawinksi J, Bocquet V, et al. Very short (15s-15s) interval-training around the critical velocity allows middle-aged runners to maintain VO2 max for 14 minutes. Int J Sports Med. 2001;(22):201-208.
- Laughlin MH and Roseguini B. Mechanisms for exercise training-induced increases in skeletal muscle blood flow capacity: differences with interval sprint training versus aerobic endurance training. J Physiol Pharmacol. 2008;(59 Suppl 7):71-88.
- Astrand I, Astrand PO, Christensen EH, et al. Intermittent muscular work. Acta Physiol Scand. 1960;(48):448-453.
- Christensen EH, Hedman R, and Saltin B. Intermittent and continuous running. (A further contribution to the physiology of intermittent work.). Acta Physiol Scand. 1960;(50):269-286.
- Billat LV. Interval training for performance: a scientific and empirical practice. Special recommendations for middle- and long-distance running. Part I: aerobic interval training. Sports Med. . 2001;(1):13-31.
- Boullosa DA, Abreu L, Varela-Sanz A, et al. Do olympic athletes train as in the Paleolithic era? Sports Med. 2013;(43):909-917.
- Faude O, Schnittker R, Schulte-Zurhausen R, et al. High intensity interval training vs. high-volume running training during pre-season conditioning in high-level youth football: a cross-over trial. J Sports Sci. 2013;(31):1441-1450.
- Tuimil JL, Boullosa DA, Fernandez-del-Olmo MA, et al. Effect of equated continuous and interval running programs on endurance performance and jump capacity. J Strength Cond Res. 2011;(25):2205-2211.
- Stoggl T and Sperlich B. Polarized training has greater impact on key endurance variables than threshold, high intensity, or high volume training. Front Physiol. 2014;(5):33.
- Bouchard C and Rankinen T. Individual differences in response to regular physical activity. Med Sci Sports Exerc. 2001;(33):S446-451.
- Baquet G, van Praagh E, and Berthoin S. Endurance training and aerobic fitness in young people. Sports Med. 2003;(33):1127-1143.
- Buchheit M. The 30-15 Intermittent Fitness Test : 10 year review. Myorobie Journal 2010;(1):http://www.martin-buchheit.net
- Bundle MW, Hoyt RW, and Weyand PG. High-speed running performance: a new approach to assessment and prediction. J Appl Physiol. 2003;(95):1955-1962.